ISSN 1080-3521
EDUCATIONAL SYNOPSES IN ANESTHESIOLOGY
and
CRITICAL CARE MEDICINE - Italy -
|
|
Copyright (C) 1996 Educational Synopses in Anesthesiology and Critical Care Medicine. All rights reserved. This on-line journal may be copied and distributed freely,providing that it is distributed in its entirety, with all author and editorial credits intact. At the end the journal information for readers is reported | |
In this issue:
1 VASCULAR ACCESS CHOICE
2 DOPPLER FLUXIMETRY & GESTATIONAL HYPERTENSION
3 INTOXICATION OF THE MONTH: Ingestion of Mandrake
4 ANESTHESIA MANUAL: Surgery of
the Upper Limbs
________________________________________________________
1 VASCULAR ACCESS CHOICE
________________________________________________________
A.BARBATI - D.LUCUGNANO
PALLIATIVE CARE UNIT - A.CARDARELLI
HOSPITAL - NAPOLI, ITALY
| Choosing the type of central venous access isn't easy because there are many indications, fields of use, and models of equipment available on the market. Proper planning of a system requires evaluation of how and why the system will be used, and for how long. The main indications are provided by oncology/hemotology, intensive care, nephrology, total parenteral nutrition, and the treatment of patients with A.I.D.S. Oncology/hemotology has given an important impetus to the development of new models of catheters and the use of new materials. The development of theraputic protocols that call for continuous administration of chemotherapy or the use of high phlebo-damaging dosages have posed the problem of such catheters remaining in situ for long periods. In addition, the treatment of patients who lead nearly normal lives at home has necessitated caution in determining the minimum dosage possible capable of improving quality of life. Other important problems are posed by immunodeficiency and coagulopathy that often accompany these pathologies or are caused by the therapy itself. However, thanks to the new technologies available it is possible to install a central venous access even in special patients such as those affected by A.I.D.S. who derive a sure and lasting benefit from it. Venous chelating therapy in hemoglobinpathic and thalassomic patients sometimes necessitates it. Therefore, a central venous device with a pump connection is indispensable. | |
| Intensive care doesn't require central venous access for very long periods, but in long-term patients protection of the veins is essential for future needs of peripheral vein access. T.P.N. is made possible by central catheters and, when they must last several months, can be conducted normally only with an adequate infusion system. In nephrology the possibility of doing hemodiaysis by means of a central venous catheter enables us to surmount the difficulties derived from the simultaneous unavailability of the fistula. |  |
| A single classification of central venous accesses is impossible so we will distinguish them according to location of the access, type of catheter, lumens, materials, and accessories. | 
|
 | The site of the access can be peripheral or central. Peripheral access usually consists of the veins of the upper limbs, while central access can consist of the jugular veins or the subclavian approached either above or below the clavate process. |
 | Installation methods call for an external metal needle (practically in disuse because of the danger of cutting the catheter itself), or an external tube. The Seldinger method that utilizes a guide in the needle permits the use of subtler needles and the positioning of even large diameter catheters with the aid of a dilator.
|
 | Different types of catheters are increasing to satisfy more specific uses. We will begin by listing the "peripherals" that call for the intubation of a vein of the upper limb: P.I.C.C. (peripherally inserted central catheter), and P.P.S. (peripheral port system). Then we will proceed to the central accesses: C.V.C. (central venous catheter), T.C.V.C. (tunnelled C.V.C.), and C.P.S. (central port system). The C.V.C. devices currently on the market provide a number of lumens from 1 to 5, or 1 - 2 lumens for high flow catheters plus an eventual third lumen of smaller diameter. |
 | Continuing technological evolution offers many materials. |
 | The ideal C.V.C. should be: biocompatible, non-thrombogen, non-degradible, chemically inert, apyrogenic, soft, solid, non-endothelial damaging, high ratio of internal/external diameter, radiopaque, resistent to infections, transparent external connections, and Luer-Look connections. |
| As for accessories we will indicate the measures which the companies develop to avoid the complications resulting from the longer and more widespread use of these protectors. We will only list a few without elaboration: | |
 | -Dacron cover for the subcutaneous stability of the catheter, anti-microb cover filled with silver salts
-Soaking the whole catheter with antibiotic (minocyclin or rifampicin)./Soaking with heparin (even though clinical studies have not demonstrated any significant action on the formation and dimensions of coagulates).
-Distal valve (Groshong) th avoid reflux of blood./Softest point for the least endothelial danger.
Establishing the system without using x-rays (Cath-Finder, Cath-Track). |
| The materials used for the implanted devices for the administration of drugs should be of high medical and mechanical quality. Among the most important we should note chemical inertia and resistence to traction, tearing, abrasion, ethylene oxide, ionizing radiation, light, heat, and aging. The medical qualities are: no acute ot chronic toxicity, not biodegradible, no pyrogens, anallergic, insoluable in organic liquids, no interaction with medications, biocompatible with the blood, tissues, and cells, and not carcinogenic. |  |
| The materials most commonly used are: polyvinylchloride (PVC), polyethylene (PE), fluoropolymers (PTFE-Teflon), polyurethane (PUR), and silicone (SI). The following are used for the port of the implantable systems: titanium, epoxic resin and titanium resin, and various plastic polymers with or without titanium.
Let's briefly analyse the main characteristics of the materials used: | |
 | -PVC is a plastic vinyl homopolymer that requires numerous additives and auxiliaries to gain the necessary characteristics. The advantages of this material consist in the wide variety of properities it can have, its solidity and low cost. The main disadvantages are: poor biocompatibility in that it can leave the additives and auxiliaries (plastics, thermal stabilizers, dyes, darkeners, lubricants, antistatics, etc.), poor compatibility with medication, and thrombogenesis. |
 | -PE is a polyolefin that is much purer than PVC. It is chemically inert, compatible with medications, light, resistent to x-rays, and economical. The disadvantages are that it is not very biocompatible since it loses its additives so its characteristics change in time, it is rigid but fragile, and it is sensitiv to UV radiation. |
 | -PUR is a class of plastic materials derived from the polyaddition of a polyisocyanate and a polyoil. Since there are many of these, a great number of polyurethanes are obtainable. Their great development is due to their interesting characteristics and the potentials of their evolution. The advantages are: purity, high biocompatibility, low thrombogenesis, softness, elasticity, thermoplasticity, and high resistence. The disadvantages are: chemical inertia is not absolute, the slight harmfulness, and the high cost. |

| -PTFE's most famous representative is Teflon. The family comes from flurocarbonate resins which are very pure, chemically inert, and anti-adherent (which makes them ideal for domestic appliances). The disadvantages are minimal biocompatibilty and rigidity. It is also harmful to the endothelium, highly thrombogenic, and creases from supports. |

| -Silicone is a synthetic elastomer with very unusual characteristics. Formulations of high molecular weight are used for catheters with the advantage of great purity, chemical inertia, hydrorepellence, excellent biocompatibility, softness, low endothelial harmfulness, very low thrombogenesis, and stability even with age. The disadvantages are that the softness presents problems for implanting, it isn't transparent, and it is expensive. |

| -Titanium is used for implantable access chambers and has the advantage of being highly biocompatible, inert, and solid. The disadvantages are that it is relatively heavy and may interfere with RMN. |
 | -Epoxic resins and plastic polymers are numerous and are being developed for their advantages: lightweight, non-interference with RMN, variety of characteristics depending on the formulation, and low cost. The disadvantages are: low biocompatibility, low chemical inertia, low solidity. It is also important to be careful about the formulation because of variable characteristics. |
| An analysis of all these facts has led to the formulation of a flow chart for a reasonable choice of the best device depending on the type of patient, and the possibilities offered by such a large variety of characteristics. | |
 | Before choosing the best venous access it is necessary to find out if the patient is affected by hemocoagulopathy, immunodeficit, whether it will be used for emergency therapy, chronic therapy, or total parenteral nutrition. |
 | Only after such considerations and by using a flow chart can we achieve the best possible use of the devices in terms of cost/benefit. |
| We hope that better education as to respect for the veins will lead to more effective treatment and less stress and suffering for the patient. | |
2 DOPPLER FLUXIMETRY & GESTATIONAL
HYPERTENSION
________________________________________________________
M. Sorrentino
Obstetric & Ginecology Division - Buccheri La Ferla Fatebenefratelli Hospital
Palermo, Italy
Doppler fluximetry is a system for the
hemodynamic study of the fetus and placenta. It is based on the
principle of sound wave transmission through the alternation of
compression and rarefication phases in the transmission media
particles with the formation of a wave. The sound frequency corresponds
to the number of compression and rarefication cycles that pass
a certain point in one second. When the sound emission source
moves in relation to the receiver the perceived frequency varies
according to the distance between emission and receiver. The Doppler
signals produce a change (Doppler shift) approaching the transducer
that is revealed on the monitor as an increase from the base line,
while signals that move away from the transducer are represented
as a decrease. There are three types of Doppler systems: continuous
wave Doppler (no longer widely used), pulsating Doppler, and color
coded Doppler. The exam is performed by positioning the sample
volume (which is the portion of space determined by the operator
from which we can evaluate the variations of frequency in the
returning echoes), on the vessel we want to analyze. The resistence
of blood flow in the vessels can be determined by the analysis
of these waves. The methods of analyzing the waves and evaluating
the flow resistence can be quantitative or qualitative, depending
on the pulsating blood flow.
The most commonly used quantitative methods are:
Systolic/diastolic ratio (S/D),
Resistence index: RI = (S/D) / S,
Pulsating index: PI = (S/D) / average.
They are all based on the relationship between systolic and diastolic flow, measured by the amplitude of the Doppler shift. The qualitative method is represented by the study of the structure of the wave which provides useful pronostic information (presence of a notch = notch on the wave profile). (Fig. 1)

|
| Figure 1 - Diastolic and systolic Notch |
In theory the principle of Doppler Fluximetry can be applied to vessels in every area of the body, but in practice its use is limited by the insufficient size of some vessels (e.g. the fetal pulmonary tree), for which a new technique has been introduced: Power Doppler, in which a color map of the energy of the Doppler signal is used instead of variations of frequency. The uterus is vascularized by the uterine arteries which originate in the anterior branch of the internal iliac artery. The radial artery originates in the arched artery which originates in the uterine artery. The radial artery is the origin of the spiral arteries which are affected by the cyclic changes of menstruation. (Fig. 2)
|
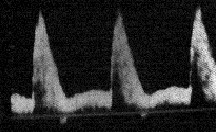
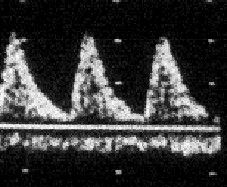
Essential information on the hemodynamic condition of the fetus and placenta is provided by Doppler fluximetry of the maternal uterine artery, which investigates the maternal side; while the fetal side can be studied in all vascular areas from the cardiac chamber to the smallest vessels. (Commonly, fluximetric evaluation is performed from the fetal umbelical vessels and the media cerebral artery.) Until recently the study of venous vessels was considered to be of secondary importance, however the demontration of venous pulsations is important because it indicates that the resistence is so high that fetal conditions are seriously compromised. The study of volumetric waves obtained from the maternal uterine artery (taken from the intersection of the external iliac vessels) or from its largest branches (RI and notch indexes used), has demontrated a reduction in flow resistence with the progress of pregnancy. When pregnancy reaches the 2nd trimester the uterous becomes a low resistence organ with a diastolic flow component. (Fig.3)
| Figure 3
Uterine artery wave of a pregnant patient : increased diastolic flow |
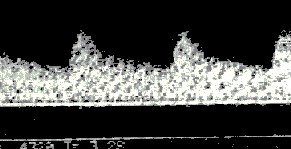
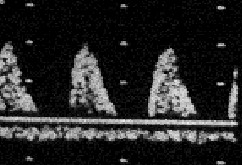
It has been demontrted the the trophoblast invades the myometrium tracts of the spiral arteries, destroying the elastic lamin and substituting itself for the soft muscle elements which causes a deficit in the ability of these vessels to contract. This diminished capacity leads to the formation of low resistence vascular systems with a characteristic continuous flow evidenced by a high diastolic component. In a normal pregnancy the S/D and RI of the uterine artery decrease significantly with the progress of the pregnancy up to 24-26 weeks, where it reaches a plateau. In the absence of this physiological decrease or in the presence of a systolic notch a higher rate of hypertensive pathology and/or IUGR has been well documented. There is also a progressive decrease in S/D and PI values (which is the index used) in the umbelical artery (taken from the intermdiate tract of the course of the funiculus), as is the case in the uterine artery in normal pregnancy, principally due to the physiological decrease in the resistence on the placental level. (Fig. 4)
| Figura 4
Umbelical artery wave of a normal pregnant patient |
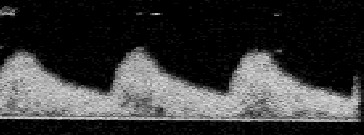
In a fetus affected by IUGR there is an increase in these indexes due to an increase in the vascular resistence on the placental level. (Fig. 5,6,7) Other explanations for these increases are the increased viscosity of the blood or an increase in arterial pressure. The fluximetric wave of the cerebral media artery (taken from its middle tract) is characterized by an absence of diastolic phase, the appearence of which indicates a condition of cerebral vessel dilation (brain sparing) and hence a compensation for a situation of initial fetal suffering.
 |  |
 |
Figura 7 Retrograde telediastolic flow |
Since fluximetry gives information on
fetal hemodynamic conditions it is used in high risk pregnancies
(hypertension, diabetes, premature birth, cardiac pathology) both
to monitor the pregnancy and to establish the timing and modality
of delivery.
Hypertension
Hypertensive disorders caused by pregnancy
are found in 5-10% of pregnant women, especially nullipare. A
woman can be hypertensive before pregnancy, or become so after
it.
| Chronic hypertension: persistent hypertension throughout pregnancy |
| Gestational hypertension: hypertension that appears after the 20th week of gestation in a pregnancy that was previously healthy. |
| Pre-eclampsia: severe gestational hypertension with significant eclampsia proteinuria |
| Eclampsia: including general hypertension and convulsions during or after pregnancy and labor, which is not due to epilepsy or other convulsive disorders |
A chronically hypertensive patient can have a superimposed pre-eclampsia. A pregnant woman is considered hypertensive if she has diastolic pressure of 110mmHg or over in a single occasion, or 90mmHg or over in two consecutive readings that are four hours or more apart. Proteinuria is considered significant when it is over 0.3 g/l in 24 hours. The definition of pre-eclampsia thatused to indicate the symptomologic series that precedes the eclamptic attack, today substitutes the EPH-gestosis, in which edema constitutes the symptomologic triade with hypertension and proteinuria and no longer appears among the classic symptoms of the disease. The pathogenic etiology of pregnancy-induced hypertension is not yet completely defined, however such patients have certain altered hemodynamic parameters such as increased vascular resistence, increased arterial pressure, decreased utero-placental circulation. The modifications associated with pre-eclampsia involve almost all the apparatus, resulting in:
-generalized vessel constriction
-decreased volemia
-reduction of renal function
-presence of fiber deposits in the glomerules and small blood vessels
-decrease in the utero-placental perfusion,
and fetal suffering.
The element that most often characterizes
the hemodynamic profile of pre-eclampsia is hypovolemia which,
along with the increase in peripheral vascular resistence, causes
renal and placental hypoperfusion. Hemorheologic modifications
(increase in hematic viscosity and changes in erythrocyte deformability),
also lead to a modification in blood flow whose normal viscosity
is the basis of ottimum placental function. Such modifications,
which are often accompanied by fibrin deposits, increase in plaque
aggregates on the arteriolar level, and increase in the production
of thrombosano - a powerful vessel constrictor - all contribute
to the increase in placental resistence. Depending on recent gains,
there can be an altered process of placentation on the basis of
those modifications with inadequate trophoblastic invasion of
the spiral arteries during the first phase of pregnancy. That
leads to a local condition of hypoxia, acidosis, accumulation
catabolites, and the imission in circulation of substances that
cause endothelial damage, which is the principle origin of the
pathogenic mechanism in hypertensive disorders in pregnancy. The
correlations between maternal hemorheologic modifications and
fetal hemodynamic parameters reveal an increase in the resistence
of uterine or umbelical arteries.
Fluximetric investigation reveals elevated
RI and PI values. Such a hemodynamic situation causes a reduction
in the supply of oxygen for the fetus and a redistribution of
fetal hematic flow, aimed at preserving circulation in vital organs.
It has been demonstrated that fetal cerebral circulation has the
characteristic of regulating itself in such a way that the cerebral
parenchyma always receives an adequate supply of nutrients even
in conditions of relative scarcity; when that mechanism deteriorates
serious damage to the SNC results. Such phenomena explain the
appearence of complications such as placental insufficiency and
IUGR. In these conditions the onset of labor is an element that
worsens tissural hypoxia because of the increased need for oxygen
in labor.